To determine the anatomical and functional state of the fetus during pregnancy, there are a number of methods, the most common of which is. It is quite informative, allows you to reach a large number of women and, most importantly, is safe.
In order to detect malformations and diseases, ultrasonic(universal rapid survey, covering more than 85% of pregnant women). It allows you to make decisions about the further management of each pregnancy, as well as identify pregnant women at risk for the development of various complications for the fetus and mother.
Ultrasound procedure ( most appropriate to carry out in the following screening terms pregnancy:
Chorion- the outer villous embryonic membrane, which, together with the wall of the uterus, later forms, thanks to which the fetus is nourished during pregnancy. Its localization gives an idea of the further localization of the placenta (what you need to know to determine the tactics of pregnancy management), and a change in thickness may indicate the presence of intrauterine infection of the embryo / fetus, as well as malnutrition of the fetus, although this indicator is also more informative in late pregnancy.
In addition, during the first, structural features of the uterus (for example, doubling of the uterus, saddle uterus) and its appendages (primarily the presence of ovarian cysts) are noted. These indicators are also important for determining further tactics of pregnancy management.
If necessary, the doctor of ultrasound diagnostics notes in the protocol the date of the repeated ultrasound control.
Deciphering the indicators of the second ultrasound at 20-24 weeks
Pregnancy 20-24 weeks optimal for studying the anatomical structures of the fetus. Identification at this time determines the further tactics of pregnancy management, and in case of a gross defect that is incompatible with life, it allows you to terminate the pregnancy. A typical ultrasound protocol at 20-24 weeks is presented in Table 5.

The structure of the ultrasound protocol can be divided into the following main groups:
- Information about the patient (name, age, the beginning of the last menstruation)
- Fetometry(measurement of the main dimensions of the fetus)
- Anatomy of the fetus (organs and systems)
- Provisional organs (temporarily existing, such as the placenta, umbilical cord, and amniotic fluid)
- Conclusion and recommendations
In this protocol, as with ultrasound at 10-14 weeks, the first day of the last menstruation is indicated, relative to which the gestational age is calculated. It also notes the number of fruits and that the fruit is alive(this is determined by the presence of and ). In the presence of two or more fruits, each is studied and described separately. Be sure to indicate (the ratio of the large part of the fetus to the entrance to the pelvis). It may be head(fetus presented with head) and (buttocks and/or legs presented). The fruit may be located transversely which should be reflected in the protocol.
Next is carried out fetometry- measurement of the main dimensions of the fetus, among which are determined: the biparietal size of the head, its circumference and fronto-occipital size, abdominal circumference, the length of the tubular bones on the left and right (femur, humerus, bones of the lower leg and forearm). The combination of these parameters makes it possible to judge the rate of fetal growth and compliance with the estimated gestational age for menstruation.
Biparietal fetal head size (BDP) measured from the outer surface of the upper contour to the inner surface of the lower contour of the parietal bones (Figure 1, line bd).
Fronto-occipital size (LZR)– distance between the outer contours of the frontal and occipital bones (Figure 1, line ac).
Cephalic index- BPR / LZR * 100% - allows you to draw a conclusion about the shape of the fetal head.
Head circumference (OH)- the circumference along the outer contour.
Measurement of head dimensions is carried out with strictly transverse ultrasound scanning at the level of certain anatomical structures of the brain (cavity of the transparent septum, cerebral peduncles and visual tubercles), as shown in the right side of Figure 1.
Figure 1 - Scheme for measuring the size of the fetal head

1 - cavity of the transparent septum, 2 - visual tubercles and legs of the brain,bd- biparietal size,ac- fronto-occipital size
The dimensions of the abdomen are measured by scanning in a plane perpendicular to the spinal column. This defines two sizes - diameter and circumference of the abdomen, measured along the outer contour. The second parameter is used more often in practice.
Further measured length of the tubular bones of the limbs: femoral, shoulder, lower leg and forearm. It is also necessary to study their structure to rule out the diagnosis. skeletal dysplasia(genetically determined pathology of bone and cartilage tissue, leading to serious disorders in the growth and maturation of the skeleton and affecting the functioning of internal organs). The study of the bones of the limbs is carried out on both sides, so as not to miss reductional malformations(that is, underdevelopment or absence of parts of the limbs on one or both sides). Percentile values of fetometric indicators are shown in Table 6.

The study fetal anatomy- one of the most important components of ultrasound at 20-24 weeks. It is in this period manifest(manifest themselves) many. The study of the anatomical structures of the fetus is carried out in the following order: head, face, spine, lungs, heart, abdominal organs, kidneys and bladder, limbs.
The study brain structures begins even when measuring the size of the head, because upon careful examination, the doctor can determine the integrity of the bone structure, the presence extracranial(outside the skull) and intracranial(intracranial) formations. The study of the cerebral hemispheres, the lateral ventricles, the cerebellum, the large cisterna, visual tubercles and the cavity of the transparent septum is carried out. The width of the lateral ventricles and the anteroposterior size of the large cistern do not normally exceed 10 mm. An increase in this indicator indicates a violation of the outflow or production of fluid and the appearance of dropsy of the brain.
The next step is studying face– the profile, eye sockets, nasolabial triangle are assessed, which makes it possible to identify anatomical defects (for example, “protrusion” of the upper jaw in case of bilateral or median facial cleft), as well as the presence of markers of chromosomal abnormalities (reduction of the length of the nasal bones, smoothed profile). When studying the eye sockets, a number of gross defects can be determined, for example, cyclopia(eyeballs are completely or partially fused and are located in the middle of the face in one eye socket), neoplasms, anophthalmia(underdevelopment of the eyeball). The study of the nasolabial triangle primarily reveals the presence of the palate.
Study spine throughout in longitudinal and transverse scanning - allows you to identify hernial protrusions, including spinabifida- spina bifida, often combined with malformations of the spinal cord.
When researching lungs their structure is studied (the presence of cystic formations can be determined), sizes, the presence of free fluid in the pleural (thoracic) cavity, neoplasms.
Further study heart for the presence of four chambers (normally, the heart consists of 2 atria and 2 ventricles), the integrity of the interventricular and interatrial septa, valves between the ventricles and the atria, as well as the presence and correct discharge / confluence of large vessels (aorta, pulmonary trunk, superior vena cava) . The very location of the heart, its size, changes in the heart bag (pericardium) are also evaluated.
When scanning organs abdominal cavity- stomach and intestines - their presence, location, size is determined, which makes it possible to indirectly judge other organs of the abdominal cavity. In addition, an increase or decrease in the size of the abdomen during fetometry indicates the presence of a pathology (for example, dropsy, hernia, hepato- and splenomegaly - an increase in the liver and spleen). Further research kidneys and bladder for their presence, shape, size, localization, structure.
The study provisional authorities allows you to indirectly judge the condition of the fetus, intrauterine infections and other conditions that require correction.
It is studied according to the following parameters:
- Localization. The doctor of ultrasound diagnostics necessarily reflects the localization of the placenta, especially its position relative to the internal pharynx of the cervix. Since with improper attachment of the placenta, for example, when it completely covers the internal os ( complete), this is accompanied by bleeding during pregnancy, and vaginal delivery is not possible. If the lower edge of the placenta is located lower than 7 cm from the internal os, ultrasound control is required at 27-28 weeks.
- Thickness. The placenta is a dynamically developing provisional organ of the fetus, therefore, during pregnancy, its thickness increases on average from 10 to 36 mm, although these values vary in a fairly large range, which is presented in table 7.
Pregnancy period, weeks | Placenta thickness, mm |
21,96 (16,7-28,6) 22,81 (17,4-29,7) 23,66 (18,1-30,7) 24,52 (18,8-31,8) 25,37 (19,6-32,9) 26,22 (20,3-34,0) 27,07 (21,0-35,1) 27,92 (21,7-36,2) 28,78 (22,4-37,3) 29,63 (23,2-38,4) 30,48 (23,9-39,5) 31,33 (24,6-40,6) 32,18 (25,3-41,6) 33,04 (26,0-42,7) 33,89 (26,8-43,8) 34,74 (27,5-44,9) 35,59 (28,2-46,0) 34,35 (27,8-45,8) 34,07 (27,5-45,5) 33,78 (27,1-45,3) 33,50 (26,7-45,0) |
After 36 weeks, the thickness of the placenta usually decreases. The discrepancy between this parameter and the normative values should alert, first of all, regarding the presence of an intrauterine infectious process, as well as the discrepancy between the nutrients supplied to the fetus and its needs.
- Structure. Normally, it is homogeneous, it should not have inclusions. Inclusions may indicate premature aging of the placenta (which can cause fetal growth retardation), heterogeneity indicates the possible presence of infection.
- The degree (stage) of maturity. The placenta changes its structure unevenly, most often this process occurs from the periphery to the center. In an uncomplicated course of pregnancy, changes go through stages from 0 to III sequentially (0 - up to 30 weeks, I - 27-36, II - 34-39, III - after 36 weeks). This indicator allows predicting the complicated course of pregnancy, the presence of syndrome (SZRP). Currently, the presence of II degree up to 32 and III degree up to 36 weeks is considered to be premature maturation of the placenta. An ultrasound assessment of the structure of the placenta is shown in Table 8.

* chorionic membrane - layer with villi facing the fetus
** parenchyma- tissue of the placenta
*** basal layer- the outer surface that the placenta adjoins the wall of the uterus
Used for evaluation amniotic fluid index. When it is determined, the uterine cavity is conditionally divided into 4 quadrants by two planes drawn through the white line of the abdomen (the connective tissue structure of the anterior abdominal wall located along the midline) vertically and horizontally at the level of the navel. Further, in each quadrant, the depth (vertical size) of the largest pocket of amniotic fluid (amniotic fluid) free from parts of the fetus is determined, all 4 values are summed up and displayed in centimeters. If the index is less than 2 cm - this is, if more than 8 cm -. This is a diagnostically significant sign of the presence of infection, malformations. Indicators of the amniotic fluid index at different stages of pregnancy are presented in Table 9.

Umbilical cord(a provisional organ that connects the embryo / fetus with the mother's body) normally contains 3 large vessels: one vein and two arteries. In many hereditary pathologies, only one umbilical artery occurs, which requires more careful management of pregnancy.
Also subject to mandatory research (for its length, which is important in the presence of a threat of termination of pregnancy), appendages(for ovarian cysts) uterine wall(if there was a caesarean section in the anamnesis, the condition of the scar is assessed).
Based on the ultrasound examination performed during pregnancy, a conclusion is made about the presence of (VLOOKUP) fetus or some other pathology and recommendations are given.
Ultrasound indicators in the third trimester
Third ultrasound at 32-34 weeks necessary to detect malformations that appear only in late pregnancy (for example, , aneurysm of the vein of Galen- violation of the structure of the vascular wall of a large cerebral vessel). It allows you to assess the functional state of the fetus, make a diagnosis syndrome (SZRP), which makes it possible to carry out a complex of necessary therapeutic measures, to identify indications for timely and careful delivery. The presence of sdfd requires mandatory monitoring after 7-10 days against the background of active therapy.
An important point is (head or), which significantly affects the method of delivery. It is also necessary to define estimated fetal weight, which should be taken into account in the tactics of further management of pregnancy and especially childbirth.
To assess the condition of the fetus in the third trimester, the definition can be used biophysical profile of the fetus during ultrasound (Table 10).

When evaluating the tabular parameters, the sum of the points is determined, on the basis of which a conclusion is made about the condition of the fetus:
- 12-8 – norm;
- 7-6 - the doubtful condition of the fetus, the possible development of complications;
- less than 5- pronounced intrauterine hypoxia(lack of oxygen supply to the fetus, leading to varying degrees of impairment of its vital functions) with a high risk perinatal losses(fetal loss between pregnancy and 168 hours after birth).
Ultrasound examination during screening periods allows to detect a large number of pathologies and take preventive measures to eliminate them as much as possible in the prenatal period, and if it is impossible to eliminate them, to reduce the consequences.
Indications for brain echography
- Prematurity.
- neurological symptoms.
- Multiple stigmas of disembryogenesis.
- Indications of chronic intrauterine hypoxia in history.
- Asphyxia in childbirth.
- Syndrome of respiratory disorders in the neonatal period.
- Infectious diseases in mother and child.
To assess the state of the brain in children with an open anterior fontanel, a sector or microconvex sensor with a frequency of 5-7.5 MHz is used. If the fontanel is closed, then you can use sensors with a lower frequency - 1.75-3.5 MHz, but the resolution will be low, which gives the worst quality of echograms. When examining premature babies, as well as for assessing surface structures (sulci and convolutions on the convexital surface of the brain, extracerebral space), sensors with a frequency of 7.5-10 MHz are used.
Any natural opening in the skull can serve as an acoustic window for studying the brain, but in most cases a large fontanelle is used, since it is the largest and last to close. The small size of the fontanel significantly limits the field of view, especially when assessing the peripheral parts of the brain.
To conduct an echoencephalographic study, the transducer is placed over the anterior fontanel, oriented so as to obtain a series of coronal (frontal) sections, and then turned 90° to perform sagittal and parasagittal scanning. Additional approaches include scanning through the temporal bone above the auricle (axial section), as well as scanning through open sutures, the posterior fontanel, and the atlanto-occipital articulation.
According to their echogenicity, the structures of the brain and skull can be divided into three categories:
- hyperechoic - bone, meninges, fissures, blood vessels, choroid plexuses, cerebellar vermis;
- medium echogenicity - parenchyma of the cerebral hemispheres and cerebellum;
- hypoechoic - corpus callosum, pons, cerebral peduncles, medulla oblongata;
- anechoic - liquor-containing cavities of the ventricles, cisterns, cavities of the transparent septum and Verge.
Normal variants of brain structures
Furrows and convolutions. The sulci appear as echogenic linear structures separating the gyri. Active differentiation of convolutions begins from the 28th week of gestation; their anatomical appearance precedes echographic imaging by 2–6 weeks. Thus, by the number and severity of the furrows, one can judge the gestational age of the child.
Visualization of the structures of the insular complex also depends on the maturity of the newborn. In very premature babies, it remains open and is presented in the form of a triangle, a flag - as a structure of increased echogenicity without the definition of furrows in it. The closure of the Sylvian furrow occurs as the formation of the frontal, parietal, occipital lobes; complete closure of the islet with a clear Sylvian furrow and vascular formations in it ends by the 40th week of gestation.
Lateral ventricles. The lateral ventricles, ventriculi lateralis, are cavities filled with cerebrospinal fluid, visible as anechoic zones. Each lateral ventricle consists of an anterior (frontal), posterior (occipital), lower (temporal) horns, a body, and an atrium (triangle) - fig. 1. The atrium is located between the body, the occipital and parietal horns. The occipital horns are difficult to visualize, their width is variable. The size of the ventricles depends on the degree of maturity of the child, with an increase in gestational age, their width decreases; in mature children, they are normally slit-like. Mild asymmetry of the lateral ventricles (difference in the size of the right and left lateral ventricles in the coronal section at the level of the foramen of Monro up to 2 mm) is quite common and is not a sign of pathology. Pathological expansion of the lateral ventricles often begins with the occipital horns, so the lack of the possibility of their clear visualization is a serious argument against expansion. We can talk about the expansion of the lateral ventricles when the diagonal size of the anterior horns on the coronal section through the foramen of Monro exceeds 5 mm and the concavity of their bottom disappears.
Rice. one. The ventricular system of the brain.
1 - interthalamic ligament;
2 - supraoptic pocket of the III ventricle;
3 - funnel-shaped pocket of the III ventricle;
5 - Monro hole;
6 - body of the lateral ventricle;
7 - III ventricle;
8 - pineal pocket of the III ventricle;
9 - glomerulus of the choroid plexus;
10 - posterior horn of the lateral ventricle;
11 - lower horn of the lateral ventricle;
12 - Sylvian plumbing;
13 - IV ventricle.
Vascular plexuses. The choroid plexus (plexus chorioideus) is a richly vascularized organ that produces cerebrospinal fluid. Sonographically, the plexus tissue appears as a hyperechoic structure. The plexuses pass from the roof of the third ventricle through the holes of Monro (interventricular holes) to the bottom of the bodies of the lateral ventricles and continue to the roof of the temporal horns (see Fig. 1); they are also present in the roof of the fourth ventricle, but are not detected echographically in this area. The anterior and occipital horns of the lateral ventricles do not contain choroid plexuses.
Plexuses usually have an even, smooth contour, but there may be irregularities and slight asymmetry. The choroid plexuses reach their greatest width at the level of the body and the occipital horn (5-14 mm), forming a local seal in the atrium region - the vascular glomerulus (glomus), which can be in the form of a finger-shaped outgrowth, be layered or fragmented. On coronal sections, the plexuses in the occipital horns look like ellipsoidal densities, almost completely filling the lumen of the ventricles. In children with a lower gestational age, the size of the plexuses is relatively larger than in full-term ones.
The choroid plexuses can be a source of intraventricular hemorrhages in full-term children, then their clear asymmetry and local seals are visible on the echograms, in the place of which cysts then form.
III ventricle. The third ventricle (ventriculus tertius) is a thin slit-like vertical cavity filled with cerebrospinal fluid, located sagittally between the thalamus above the Turkish saddle. It connects to the lateral ventricles through the foramen of Monro (foramen interventriculare) and to the IV ventricle through the Sylvian aqueduct (see Fig. 1). The supraoptic, funnel-shaped and pineal processes give the third ventricle a triangular appearance on the sagittal section. On the coronal section, it is visible as a narrow gap between the echogenic visual nuclei, which are interconnected by an interthalamic commissure (massa intermedia) passing through the cavity of the third ventricle. In the neonatal period, the width of the third ventricle in the coronal section should not exceed 3 mm, in infancy - 3-4 mm. The clear outlines of the third ventricle on the sagittal section indicate its expansion.
Sylvius aqueduct and IV ventricle. The aqueduct of Sylvius (aquaeductus cerebri) is a thin canal connecting the III and IV ventricles (see Fig. 1), rarely visible on ultrasound in standard positions. It can be visualized on the axial section as two echogenic dots against the background of hypoechoic cerebral peduncles.
IV ventricle (ventriculus quartus) is a small diamond-shaped cavity. On echograms in a strictly sagittal section, it looks like a small anechoic triangle in the middle of the echogenic medial contour of the cerebellar vermis (see Fig. 1). Its anterior border is not clearly visible due to the hypoechogenicity of the dorsal part of the bridge. The anteroposterior size of the IV ventricle in the neonatal period does not exceed 4 mm.
Calloused body. The corpus callosum (corpus callosum) on the sagittal section looks like a thin horizontal arcuate hypoechoic structure (Fig. 2), bounded above and below by thin echogenic strips resulting from reflection from the corpus callosum (from above) and the lower surface of the corpus callosum. Immediately below it are two sheets of a transparent partition, limiting its cavity. On the frontal section, the corpus callosum looks like a thin narrow hypoechoic strip forming the roof of the lateral ventricles.

Rice. 2. The location of the main brain structures on the median sagittal section.
1 - varolian bridge;
2 - prepontine cistern;
3 - interpeduncular cistern;
4 - transparent partition;
5 - legs of the arch;
6 - corpus callosum;
7 - III ventricle;
8 - cistern of the quadrigemina;
9 - legs of the brain;
10 - IV ventricle;
11 - a large tank;
12 - medulla oblongata.
The cavity of the transparent septum and the cavity of Verge. These cavities are located directly under the corpus callosum between the sheets of the transparent septum (septum pellucidum) and are limited by glia, not ependyma; they contain fluid but do not connect to either the ventricular system or the subarachnoid space. The cavity of the transparent septum (cavum cepti pellucidi) is located anterior to the fornix of the brain between the anterior horns of the lateral ventricles, the Verge cavity is located under the corpus callosum between the bodies of the lateral ventricles. Sometimes, normally, dots and short linear signals originating from the subependymal median veins are visualized in the sheets of the transparent septum. On the coronal section, the cavity of the septum pellucidum looks like a square, triangular or trapezoidal anechoic space with a base under the corpus callosum. The width of the cavity of the transparent septum does not exceed 10-12 mm and is wider in premature infants than in full-term ones. Verge's cavity, as a rule, is narrower than the cavity of the transparent septum and is rarely found in full-term children. These cavities begin to obliterate after 6 months of gestation in the dorsoventral direction, but there are no exact dates for their closure, and both of them can be found in a mature child at the age of 2-3 months.
Basal nuclei, thalamus and internal capsule. The optic nuclei (thalami) are spherical hypoechoic structures located on the sides of the cavity of the transparent septum and forming the lateral borders of the third ventricle on coronal sections. The upper surface of the gangliothalamic complex is divided into two parts by the caudothalamic notch - the anterior one belongs to the caudate nucleus, the posterior one to the thalamus (Fig. 3). The visual nuclei are connected to each other by an interthalamic commissure, which becomes clearly visible only with the expansion of the third ventricle both on the frontal (in the form of a double echogenic transverse structure) and in the sagittal sections (in the form of a hyperechoic dot structure).

Rice. 3. The relative position of the structures of the basal-thalamic complex on the parasagittal section.
1 - shell of the lenticular nucleus;
2 - pale ball of the lenticular nucleus;
3 - caudate nucleus;
4 - thalamus;
5 - inner capsule.
The basal ganglia are subcortical collections of gray matter located between the thalamus and the insula of Rayleigh. They have similar echogenicity, which makes them difficult to differentiate. Parasagittal section through the caudothalamic notch is the most optimal approach for detecting the thalamus, the lentiform nucleus consisting of the shell (putamen), and the pale ball (globus pallidus), and the caudate nucleus, as well as the internal capsule - a thin layer of white matter that separates the nuclei of the striatum bodies from the thalamus. A clearer visualization of the basal nuclei is possible when using a 10 MHz probe, as well as in pathology (hemorrhage or ischemia) - as a result of neuronal necrosis, the nuclei acquire increased echogenicity.
germinal matrix is an embryonic tissue with high metabolic and fibrinolytic activity, producing glioblasts. This subependymal plate is most active between the 24th and 34th weeks of gestation and is an accumulation of fragile vessels, the walls of which are devoid of collagen and elastic fibers, are easily ruptured and are a source of peri-intraventricular hemorrhages in preterm infants. The germinal matrix lies between the caudate nucleus and the lower wall of the lateral ventricle in the cau- thalamic notch, and looks like a hyperechoic strip on echograms.
Cisterns of the brain. Cisterns are spaces containing cerebrospinal fluid between brain structures (see Fig. 2), which may also contain large vessels and nerves. Normally, they are rarely seen on echograms. When enlarged, the cisterns look like irregularly delineated cavities, which indicates a proximally located obstruction to the flow of cerebrospinal fluid.
The large cistern (cisterna magna, c. cerebromedullaris) is located under the cerebellum and medulla oblongata above the occipital bone, normally its upper-lower size on the sagittal section does not exceed 10 mm. The pontine cistern is an echogenic area above the pons in front of the cerebral peduncles, under the anterior pocket of the third ventricle. It contains a bifurcation of the basilar artery, which causes its partial echo density and pulsation.
Basal (c. suprasellar) cistern includes interpeduncular, c. interpeduncularis (between the legs of the brain) and chiasmatic, c. chiasmatis (between the optic chiasm and the frontal lobes) cisterns. The cisterna decussation looks like a pentagonal echo-dense zone, the corners of which correspond to the arteries of the circle of Willis.
The cistern of the quadrigemina (c. quadrigeminalis) is an echogenic line between the plexus of the third ventricle and the cerebellar vermis. The thickness of this echogenic zone (normally not exceeding 3 mm) may increase with subarachnoid hemorrhage. In the region of the cistern of the quadrigemina, there may also be arachnoid cysts.
Bypass (c. ambient) cistern - carries out lateral communication between the prepontine and interpeduncular cistern in front and the cistern of the quadrigemina behind.
Cerebellum(cerebellum) can be visualized through both the anterior and posterior fontanel. When scanning through a large fontanelle, the image quality is the worst due to the long distance. The cerebellum consists of two hemispheres connected by a worm. The hemispheres are slightly echogenic, the worm is partially hyperechoic. On the sagittal section, the ventral part of the worm looks like a hypoechoic letter "E" containing cerebrospinal fluid: at the top - the quadrigeminal cistern, in the center - the IV ventricle, below - a large cistern. The transverse size of the cerebellum directly correlates with the biparietal diameter of the head, which makes it possible to determine the gestational age of the fetus and newborn based on its measurement.
The cerebral peduncles (pedunculus cerebri), the pons (pons) and the medulla oblongata (medulla oblongata) are located longitudinally anterior to the cerebellum and look like hypoechoic structures.
Parenchyma. Normally, there is a difference in echogenicity between the cerebral cortex and the underlying white matter. The white matter is slightly more echogenic, possibly due to the relatively larger number of vessels. Normally, the thickness of the cortex does not exceed a few millimeters.
Around the lateral ventricles, predominantly over the occipital and less commonly over the anterior horns, preterm infants and some full-term infants have a halo of increased echogenicity, the size and visualization of which depend on gestational age. It can persist up to 3-4 weeks of life. Normally, its intensity should be lower than that of the choroid plexus, the edges should be fuzzy, and the location should be symmetrical. With asymmetry or increased echogenicity in the periventricular region, an ultrasound study of the brain in dynamics should be performed to exclude periventricular leukomalacia.
Standard echoencephalographic sections
Coronal slices(Fig. 4). First cut passes through the frontal lobes in front of the lateral ventricles (Fig. 5). In the middle, the interhemispheric fissure is determined in the form of a vertical echogenic strip separating the hemispheres. When it expands, a signal from the crescent of the brain (falx) is visible in the center, which is not visualized separately in the norm (Fig. 6). The width of the interhemispheric fissure between the gyri does not normally exceed 3-4 mm. On the same section, it is convenient to measure the size of the subarachnoid space - between the lateral wall of the superior sagittal sinus and the nearest gyrus (sinocortical width). To do this, it is desirable to use a sensor with a frequency of 7.5-10 MHz, a large amount of gel and very carefully touch the large fontanelle without pressing on it. The normal size of the subarachnoid space in full-term children is up to 3 mm, in premature babies - up to 4 mm.

Rice. four. Planes of coronal scanning (1-6).

Rice. 5. Echogram of the brain of a newborn, the first coronal section through the frontal lobes.
1 - eye sockets;
2 - interhemispheric fissure (not expanded).


Rice. 6. Measurement of the width of the subarachnoid space and the width of the interhemispheric fissure on one or two coronal sections - scheme (a) and echogram of the brain (b).
1 - superior sagittal sinus;
2 - the width of the subarachnoid space;
3 - width of the interhemispheric fissure;
4 - crescent of the brain.
Second cut is performed through the anterior horns of the lateral ventricles anterior to the foramina of Monro at the level of the cavity of the transparent septum (Fig. 7). Frontal horns that do not contain CSF are visualized on both sides of the interhemispheric fissure as echogenic stripes; in the presence of CSF in them, they look like anechoic structures, similar to boomerangs. The roof of the anterior horns of the lateral ventricles is represented by a hypoechoic strip of the corpus callosum, and between their medial walls there are sheets of a transparent septum containing a cavity. On this section, the shape is evaluated and the width of the cavity of the transparent partition is measured - the maximum distance between its walls. The lateral walls of the anterior horns form the basal nuclei - directly under the bottom of the horn - the head of the caudate nucleus, laterally - the lenticular nucleus. Even more lateral on this section, on both sides of the cisterna decussation, the temporal lobes are determined.

Rice. 7. Echogram of the brain, second coronal section through the anterior horns of the lateral ventricles.
1 - temporal lobes;
2 - Sylvian fissure;
3 - cavity of a transparent partition;
4 - anterior horn of the lateral ventricle;
5 - corpus callosum;
6 - interhemispheric fissure;
7 - caudate nucleus;
8 - thalamus.
Third coronal section passes through the holes of Monro and III ventricle (Fig. 8). At this level, the lateral ventricles connect with the third ventricle through the interventricular foramina (Monroe). The holes themselves are not normally visible, but the choroid plexuses passing through them from the roof of the third ventricle to the bottom of the lateral ventricles look like a hyperechoic Y-shaped structure located along the midline. Normally, the third ventricle may also not be visualized; when it is enlarged, its width is measured between the medial surfaces of the thalamus, which are its lateral walls. The lateral ventricles on this section are seen as slit-like or boomerang-shaped anechoic structures (Fig. 9), the width of which is measured diagonally (normally up to 5 mm). The cavity of the transparent septum on the third section in some cases still remains visible. Below the third ventricle, the brain stem and pons are visualized. Laterally from the third ventricle - the thalamus, the basal nuclei and the islet, over which a Y-shaped thin echogenic structure is defined - the Sylvian fissure containing the pulsating middle cerebral artery.

Rice. eight. Echogram of the brain, the third coronal section through the holes of Monro.
1 - III ventricle;
2 - choroid plexuses in the interventricular canals and the roof of the third ventricle and the fornix of the brain;
3 - cavity of the lateral ventricle;
4 - corpus callosum;
5 - caudate nucleus;
6 - thalamus.

Rice. 9. The relative position of the central brain structures on two to four coronal sections.
1 - III ventricle;
2 - cavity of a transparent partition;
3 - corpus callosum;
4 - lateral ventricle;
5 - caudate nucleus;
6 - leg of the fornix of the brain;
7 - thalamus.
On the fourth cut(through the bodies of the lateral ventricles and the posterior section of the third ventricle) are visible: interhemispheric fissure, corpus callosum, ventricular cavities with choroid plexuses in their bottom, thalamus, Sylvian fissures, vertically located hypoechoic brain legs (below the thalamus), the cerebellum, separated from the brain legs by hyperechoic bait (Fig. 10). A large cistern can be visualized downward from the cerebellar vermis. In the region of the middle cranial fossa, a site of pulsation is visible, originating from the vessels of the circle of Willis.

Rice. ten. Echogram of the brain, the fourth coronal section through the bodies of the lateral ventricles.
1 - cerebellum;
2 - vascular plexuses in the lateral ventricles;
3 - bodies of the lateral ventricles;
4 - Verge cavity.
Fifth cut passes through the bodies of the lateral ventricles and the choroid plexuses in the region of the glomus, which on the echograms almost completely fill the cavities of the lateral ventricles (Fig. 11). On this section, a comparison is made of the density and size of the choroid plexuses on both sides to exclude hemorrhages. In the presence of the Verge cavity, it is visualized between the lateral ventricles in the form of a rounded anechoic formation. Inside the posterior cranial fossa, the cerebellum is visualized with an average echogenicity, above its insignia is the echogenic cistern of the quadrigemina.

Rice. eleven. Echogram of the brain, the fifth coronal section through the choroid plexus glomus - choroid plexuses in the area of the atria, completely fulfilling the lumen of the ventricles (1).
Sixth, the last, coronal section is performed through the occipital lobes above the cavities of the lateral ventricles (Fig. 12). The interhemispheric fissure with furrows and convolutions is visualized in the middle, on both sides of it there are cloud-like periventricular seals, which are more pronounced in premature babies. On this section, the symmetry of these seals is evaluated.

Rice. 12. Echogram of the brain, sixth coronal section through the occipital lobes above the lateral ventricles.
1 - normal periventricular seals;
2 - interhemispheric fissure.
Sagittal slices(Fig. 13). mid-sagittal section(Fig. 14) allows visualization of the corpus callosum in the form of a hypoechoic arch, immediately below it is the cavity of the transparent septum (under its anterior sections) and the Verge cavity connected to it (under the ridge). A pulsating structure passes near the knee of the corpus callosum - the anterior cerebral artery, which goes around it and runs along the upper edge of the body. Above the corpus callosum there is a corpus callosum. Between the cavities of the transparent septum and Verge, an arcuate hyperechoic strip is determined, originating from the choroid plexus of the third ventricle and the fornix of the brain. Below is a hypoechoic triangular third ventricle, the contours of which are normally not clearly defined. With its expansion in the center, you can see the interthalamic adhesion in the form of a hyperechoic point. The posterior wall of the third ventricle is made up of the pineal gland and the quadrigemnal plate, behind which the quadrigemnal cistern can be seen. Immediately below it, in the posterior cranial fossa, a hyperechoic cerebellar vermis is determined, on the anterior part of which there is a triangular notch - the IV ventricle. The pons, cerebral peduncles, and medulla oblongata lie anterior to the fourth ventricle and are seen as hypoechoic masses. On this section, a large cistern is measured - from the lower surface of the worm to the inner surface of the occipital bone - and the depth of the IV ventricle is measured. 5 - corpus callosum;
6 - the cavity of the transparent partition;
7 - legs of the brain;
8 - a large tank;
9 - Verge cavity;
10 - corpus callosum;
11 - cavity of a transparent partition;
12 - III ventricle.
With a slight deviation of the sensor to the left and right, parasagittal section through the caudothalamic notch (the location of the germinal matrix in premature babies), on which its shape is assessed, as well as the structure and echogenicity of the gangliothalamic complex (Fig. 15).

Rice. fifteen. Echogram of the brain, parasagittal section through the caudo-thalamic notch.
1 - choroid plexus of the lateral ventricle;
2 - cavity of the lateral ventricle;
3 - thalamus;
4 - caudate nucleus.
Next parasagittal section is performed through the lateral ventricle on each side so as to obtain its complete image - the frontal horn, body, occipital and temporal horns (Fig. 16). In this plane, the height of various sections of the lateral ventricle is measured, the thickness and shape of the choroid plexus are assessed. Above the body and the occipital horn of the lateral ventricle, the homogeneity and density of the periventricular substance of the brain is assessed, comparing it with the density of the choroid plexus.
Rice. 17. Echogram of the brain, parasagittal section through the temporal lobe.
1 - temporal lobe of the brain;
2 - Sylvian fissure;
3 - parietal lobe.
If any deviations are determined on the received echograms in the coronal section, then they must be confirmed in the sagittal section, and vice versa, since artifacts can often occur.
axial scan. An axial cut is made by placing the transducer horizontally over the ear. At the same time, the legs of the brain are visualized as a hypoechoic structure that looks like a butterfly (Fig. 18). Between the legs, often (unlike coronal and sagittal sections), an echogenic structure is visible, consisting of two points - the Sylvian aqueduct, anterior to the legs - the slit-like III ventricle. On the axial section, the walls of the third ventricle are clearly visible, in contrast to the coronal one, which makes it possible to more accurately measure its size with a slight expansion. When the probe is tilted towards the cranial vault, the lateral ventricles are visible, which makes it possible to estimate their size when the large fontanel is closed. Normally, parenchyma of the brain is closely adjacent to the bones of the skull in mature children; therefore, the separation of echo signals from them in the axial section suggests the presence of pathological fluid in the subarachnoid or subdural spaces.

Rice. eighteen. Echogram of the brain, axial section at the level of the base of the brain.
1 - cerebellum;
2 - Sylvian water supply;
3 - legs of the brain;
4 - Sylvian fissure;
5 - III ventricle.
Data from an echographic study of the brain can be supplemented by the results of a Doppler assessment of cerebral blood flow. This is desirable, since in 40-65% of children, despite severe neurological disorders, the data of the echographic examination of the brain remain normal.
The brain is supplied with blood by branches of the internal carotid and basilar arteries, which form the circle of Willis at the base of the brain. The direct continuation of the internal carotid artery is the middle cerebral artery, the smaller branch is the anterior cerebral artery. The posterior cerebral arteries branch off from the short basilar artery and communicate with branches of the internal carotid via the posterior communicating arteries. The main cerebral arteries - the anterior, middle and posterior, form an arterial network with their branches, from which small vessels that feed the cortex and white matter of the brain penetrate into the medulla.
Doppler examination of blood flow is carried out in the largest arteries and veins of the brain, trying to position the ultrasound sensor so that the angle between the ultrasound beam and the axis of the vessel is minimal.
anterior cerebral artery visualized on the sagittal section; to obtain blood flow indicators, a volume marker is placed in front of the knee of the corpus callosum or in the proximal part of the artery before it bends around this structure.
For the study of blood flow internal carotid artery on the parasagittal section, its vertical part is used immediately after exiting the carotid canal above the level of the Turkish saddle.
basilar artery examined in the median sagittal section in the region of the base of the skull immediately in front of the bridge a few millimeters behind the location of the internal carotid artery.
Middle cerebral artery determined in the Sylvian fissure. The best angle for its insonation is achieved with an axial approach. The vein of Galen is visualized on a coronal section under the corpus callosum along the roof of the third ventricle.
BRAIN AND SPINE
In clinical practice, the technique of 4 horizontal planes is used.
The first scanning plane is used to evaluate the lateral ventricles of the brain. To identify ventriculomegaly and hydrocephalus, the width of the lateral ventricles should be measured. The threshold value above which the diagnosis of ventriculomegaly is made is 10 mm.
The second scanning plane passes through the frontal and occipital horns of the lateral ventricles. When evaluating it, it should be remembered that in many cases, the expansion of the ventricular system of the fetal brain begins with the posterior horns of the lateral ventricles. Therefore, their evaluation should be given special attention. With normal fetal development, their width is up to 32 weeks. pregnancy should not exceed 10 mm..
The third axial plane passes at the level of the optimal measurement of the biparietal and fronto-occipital dimensions of the head. In this plane, the brain peduncles and visual tubercles (thalamus) are clearly defined, forming the quadruple, and between them is the third ventricle. The width of the third ventricle normally varies from 1 to 2 mm in terms of 22 to 28 weeks. pregnancy.
On both sides of the thalamus are the gyri of the hippocampus, represented by rounded spaces, medially limited by cisterns, and laterally by the lateral ventricles.
Anterior to the thalamus are the anterior horns of the lateral ventricles, which are separated by a cavity of the transparent septum. Visualization of the cavity of the transparent septum is of fundamental importance for the exclusion of various malformations of the brain and, first of all, holoprosencephaly.
To assess the brain structures located in the posterior cranial fossa, the sensor must be deployed and shifted posteriorly from the plane in which the main dimensions of the fetal head are determined. At the same time, the hemispheres and the cerebellar vermis are consistently studied throughout, as well as the large cistern of the brain (Fig. 62). This section is used not only to exclude Dandy-Walker syndrome, which is characterized by a defect in the cerebellar vermis, but also, if necessary, to determine the transverse size of the cerebellum (Fig. 6.3). Hypoplasia of the cerebellum is established in cases where its transverse diameter is below the 5th percentile.
The large cistern of the brain is included in the protocol of the anatomical structures of the fetus, which are subject to mandatory assessment during screening echography in the II trimester, because. its expansion is regarded as a HA echomarker. The expansion of a large tank is diagnosed when its width exceeds the 95th percentile of standard values. The maximum size of a large tank does not exceed 11mm.
This technique, in addition to those described above, includes the sagittal and coronal brain scanning planes.
Sagittal scanning planes are obtained by scanning the fetal head along the anteroposterior axis (Fig. 6.5). Scanning in this plane is the most informative for the exclusion or establishment of agenesis of the corpus callosum. However, it should be noted that in order to obtain sagittal planes, sufficient practical experience of the researcher is required, since often there are certain technical difficulties due to the “uncomfortable” position of the fetus for research.
To exclude hypoplasia / dysplasia of the corpus callosum, its length and thickness are assessed during sagittal scanning, as well as the width, which is determined in the coronal plane. Coronal planes are obtained by scanning the fetal head along the lateral-lateral axis (Fig. 6.6). In anterior coronal section, the corpus callosum is visualized as an echo-negative formation between the anterior horns of the lateral ventricles and the interhemispheric fissure. In addition to assessing the corpus callosum, coronal planes are of great help in establishing the lobar form of holoprosencephaly, in which the anterior horns of the lateral ventricles merge.
Furrows and convolutions of the telencephalon are visualized in different scanning planes. The number of determined furrows increases with increasing gestational age. However, at present, reliable criteria for diagnosing their pathology have not been developed.
An important additional value for congenital malformations of the brain in the fetus is scanning in the CFM mode, which allows you to evaluate almost all the main vessels of the brain and establish the vascular genesis of the detected defects,
Spine the fetus must be evaluated throughout both the longitudinal and transverse planes. The frontal scanning plane is of great diagnostic value, when with spina bifida it is possible to visualize the absence of the posterior arches of the vertebrae, skin and muscles above the defect. The sagittal plane is used to assess spinal curvatures, which serve as an indirect sign of spina bifida, and in cases of large hernial formations with an open defect, to assess the extent of the lesion. Scanning in the transverse plane makes it possible to assess the integrity of the vertebral rings that are broken when spina bifida is closed.
Fetal CNS anomalies
Congenital malformations of the central nervous system of the fetus in terms of frequency of occurrence occupy one of the leading places in the population, accounting for 10 to 30% of all malformations, dominating in their structure.
Recent years have been marked by the growing interest of researchers in the study of the CNS in the fetus, and this is not accidental, since the incidence and mortality due to congenital brain defects currently occupies one of the first places among all malformations in infancy. In our opinion, one of the main reasons for this situation is the lateness of detection and the difficulty of accurate differential diagnosis of a number of nosological forms of congenital malformations of the brain in the fetus.
Anomalies in the development of the central nervous system is a large group of diseases caused by various causes and having a different prognosis for life and health. Some congenital malformations of the central nervous system are incompatible with life, other anomalies lead to severe neurological disorders and disability. In rare cases, CNS anomalies are subject to intrauterine treatment.
Anencephaly and acrania
Anencephaly- is one of the most common malformations of the central nervous system, in which the hemispheres of the brain and the vault of the skull are absent. At exencephaly there are also no bones of the cranial vault, but there is a fragment of brain tissue. Acrania characterized by the absence of the cranial vault, in the presence of an abnormally formed brain. The frequency of anencephaly is 1 case per 1000 newborns. Acrania is rarer than anencephaly.
Anencephaly is the result of failure to close the rostral neuropore within 28 days of fertilization. The pathological basis of acrania is unknown. Dynamic ultrasonic researches have allowed to establish that acrania, exencephaly and anencephaly are stages of development of one defect. This probably explains the fact that the frequency of exencephaly in early pregnancy exceeds the frequency of anencephaly and, conversely, anencephaly dominates over acrania and exencephaly in the II and III trimesters of pregnancy.
In an ultrasound examination of the fetus, the diagnosis of anencephaly is established when the absence of the bones of the brain skull and brain tissue is detected (Fig. 6.8). In most cases, an irregularly shaped heterogeneous structure is visualized above the orbits, which is a vascular malformation of the primary brain. The diagnosis of acrania is made in cases where the fetal brain is not surrounded by a bony vault (Fig. 6.9).
The differential diagnosis of anencephaly and exencephaly in most cases, especially in early pregnancy, presents significant difficulties. A clear identification of a fragment of brain tissue suggests the presence of exencephaly. Significant assistance in the differential diagnosis of these defects is provided by scanning in the TsDK mode. With anencephaly, the picture of the vascular system of the brain is absent due to occlusion at the level of the internal carotid arteries. Polyhydramnios can be diagnosed in both anencephaly and acrania.
Anencephaly can be diagnosed in the first trimester of pregnancy using a transvaginal examination, although it is difficult to distinguish the altered primary brain from the normal brain in the early stages. The earliest diagnosis of acrania, according to the literature, was made in 11 weeks using transvaginal echography. Due to the fact that the bones of the cranial vault of the fetus in terms of 10-11 weeks. are only partially calcified, the diagnosis of acrania must be made with caution.
Anencephaly and acrania are malformations of a multifactorial nature. Anencephaly can be part of the amniotic band syndrome (Fig. 3.93), combined with chromosomal aberrations (trisomy 18, ring chromosome 13), occur as a result of chemotherapy, against the background of maternal diabetes and hyperthermia. Anencephaly is part of Meckel-Gruber syndrome and hydrolethal syndrome. Anencephaly is often associated with cleft lip and palate, ear and nose abnormalities, heart defects, gastrointestinal and genitourinary pathology. A combination of acrania with LL-amelia syndrome has been described.
Prenatal examination for the diagnosis of anencephaly/acrania/exencephaly should include karyotyping and careful ultrasonography.
The described malformations are absolutely lethal malformations. If the patient wishes to prolong the pregnancy; delivery should be carried out in the interests of the mother, without expanding the indications for caesarean section. In these cases, parents should be warned that 50% of fetuses with anencephaly will be born alive, 66% of them will live for several hours, some may live for a week.
Cephalocele
A cephalocele is an exit of the meninges through a defect in the bones, skull. In cases where the hernial sac includes brain tissue, the anomaly is called an encephalocele. Most often, defects are located in the back of the head, but can also be detected in other departments (frontal, parietal, nasopharyngeal) (Fig. 6.11). The frequency of occurrence of the anomaly is 1 case per 2000 live births.
Antipyretics for children are prescribed by a pediatrician. But there are emergency situations for fever when the child needs to be given medicine immediately. Then the parents take responsibility and use antipyretic drugs. What is allowed to give to infants? How can you bring down the temperature in older children? What medicines are the safest?
Hydrocephalus is the accumulation of fluid from the spinal cord to the brain, including its ventricles. This factor is accompanied. This disease may be caused by an infection or another cause. The picture of this manifestation is as follows: a large amount of fluid leaves the spinal cord, which is later retained in the brain. In total there are 2 classes of this disease:
In the case of a conventional 20 week ultrasound, we will not look for anything specific, we rule out that the fetus has an unexpected and unexpected anomaly. For this, it is fundamental that the sonographer has a predetermined schema that he uses to examine in a regulated and thorough manner all the structures of the fetus, following a predetermined scenario. In general terms, the steps that are followed in the study of the fetus are as follows.
Determining the number and position of the fetus or fetus within the maternal abdomen is an important step in allowing the various structures of the fetus to be found. Determination of the mobility and viability of the fetus. Fetal measurements to know the time of pregnancy and be able to determine changes in growth. The most common measures are the biparietal diameter, which measures the distance between the parietal bones of the skull, the perimeter or circumference of the abdomen, and the length of the femur. Each of these measures is compared with a reference table in weeks and with an average value of three times the calculated time of pregnancy.
- primary, resulting from congenital anomalies;
- secondary, acquired in the womb when the fetus is infected.
The disease is classified in the following areas:
- acquired pathology;
- congenital disease;
- open, or communicating, hydrocephalus;
- closed, or occlusive, hydrocephalus;
- caused by atrophy of brain cells;
- normotensive, or normal pressure.
Hydrocephalus of the brain in the fetus occurs due to many factors, but still, these are mostly infections that enter the mother's body. And the sooner this happens, the worse for the future baby.
Systematic study of fetal anatomy. Assessment of cord placenta and amniotic fluid. It is necessary to determine the morphology and insertion of the placenta, it is necessary to visualize the cord, place it in the placenta and check the amount of amniotic fluid. Imaging of the uterus and maternal ovaries to rule out fibroids, cysts, or other abnormalities.
In the head we have to evaluate its shape and integrity; inside the skull we evaluate the encephalic structures, the cerebellum and the cisna magna. The face is scanned in front and profile to evaluate the lips, jaw, nose and eyes. In the chest, you should evaluate its shape and size and the appearance of the lungs and diaphragm.
However, the basic logic of neuroanatomy is simple. The brain is divided into wolves. Wolves are still subdivided into prominences called turns and depressions called grooves and fissures. This limits areas of great importance for the study of the neurology of vision.
The encephalic trunk contains three parts - mesencephalin, bridge and bulb. Pituitary tumors usually compress or may damage the optic chiasm. The arterial cycle is also called the Willis cycle, located on the bridge, in the format of spiders, it can be said that the "spider nose" fits into the pituitary ulcer.
If there are infectious diseases, then it is best to carry out treatment before the start of pregnancy planning, since many drugs are contraindicated during gestation. The bypass procedure for a woman should also be carried out before the conception of a baby. Preventive measures also include a scheduled ultrasound examination.
To make learning easier, dear student, since neuroanatomy usually scares you, you can use a little imagination and even some memory games. What matters is that you store the information. The neuro-optician should have this information archived and accessed with every neurological image analysis. A ferocious spider lives in the brain.
Visual neurorehabilitation - the latest methods. They act on the subjective and objective plane, while improving the internal and external perception. Beginning with the release of the "Muscular Arm of the Eyes", neuro-rehabilitation techniques promote deep brain relaxation that creates an inner serenity and peace that makes us see with clarity and insight the events of our day. When we achieve this inner peace, we experience a psychological and emotional well-being that brings us into balance.
) is characterized as a symptom complex with pathological accumulation of cerebrospinal fluid under the membranes of the brain and / or in its cavities (ventricles), and is accompanied by increased intracranial pressure. The causes of hydrocephalus in the fetus are of infectious and non-infectious origin. Pathology occurs due to excessive production of cerebrospinal fluid or violations of its outflow.
Dropsy is classified into:
primary - the result of birth defects and genetic abnormalities;
secondary - due to intrauterine infection.
We immediately feel free from the old ties of addiction that have made our relationships with others violent and unsatisfactory. The vision of meditation reduces the gaps in our personality and reveals to us the existence of an "inner compass" that can visually show us our emotional and practical decisions.
These treatments are already available in Brazil, brought from Europe by a professor. They are beneficial in the physical and energetic aspect. They deactivate and activate the chakras, adjusting our biological clock while combating insight and inertia. By increasing the sensitivity of the senses, improving and expanding their perceptual capacity, they lead us to a touching and emotional perception of many precious subtleties of life that have eluded our senses.
The main causes of hydrocephalus in the fetus
There are many factors contributing to the disease, but infectious agents that enter the baby's body from the mother play a special role. The earlier the infection occurs, the more insidious the consequences.
The basic causes of fetal hydrocephalus during pregnancy include:
1. Infections of the mother that are sexually transmitted.
Syphilis - intrauterine infection of a baby with syphilis leads to the occurrence of congenital defects of the nervous system, possible ones include dropsy of the brain. Ureaplasmosis - its role in the occurrence of hydrocephalus is under discussion, however, in many women diagnosed with fetal hydrocephalus after abortion, the presence of the causative agent of ureaplasmosis is confirmed. Chlamydia causes congenital malformations of the eyes and anomalies in the development of the nervous system.
2. TORCH infection in the mother.
Infection with toxoplasmosis occurs by eating undercooked meat and by contact with domestic and wild cats. Of particular danger is infection in early pregnancy, which leads to serious brain damage.
Rubella - the causative agent when it enters the body of a pregnant woman who has not had rubella, in the first weeks causes the death of the embryo. Infection at a later date threatens to damage the fetal brain and, possibly, the development of hydrocephalus.
Herpes infection - there is a high risk (more than 40%) of infection of the fetus from an infected mother. In newborns, lesions of the nervous system, skin, eyes, etc. are noted;
Cytomegalovirus infection - cytomegalovirus has a high affinity for the cells of the nervous system and causes mainly abnormalities in the development of the fetal brain, as an example - dropsy of the brain.
3. Congenital pathology of the baby.
Chiari Syndrome is a brain developmental disorder in which the brainstem and cerebellum descend into the foramen magnum, and the circulation of cerebrospinal fluid is disturbed. According to new data, the disease occurs due to the rapid increase in the size of the brain, which does not correspond to the size of the skull.
Edwards syndrome is classified as a chromosomal disorder, more common among girls, characterized by multiple lesions of organs and systems (including hydrocephalus), children are not viable and die in the first months of life.
Narrowing of the cerebral aqueduct, belongs to congenital damage, free flow of cerebrospinal fluid in bad habits and negative factors to give birth to a healthy baby.
Methods for diagnosing fetal hydrocephalus during pregnancy
The main method for diagnosing cerebral hydrocephalus in the fetus is ultrasound. The baby's head is measured with a transverse scan. The main criteria for the fetus on ultrasound include the width of the lateral ventricles, which normally should not exceed 10 mm. Diagnosis is carried out starting from the 17th week, a second study is carried out at 20–22 weeks of pregnancy, however, the average time when the pathology is visualized in most cases is 26 weeks. 
Another method for determining whether there is fetal hydrocephalus during pregnancy is echography. However, it is only available in large diagnostic centers.
Possible prognosis and consequences of fetal hydrocephalus
The consequences can be different and depend on the size of the violation and associated developmental defects. In the case when the size of the lateral ventricles does not exceed 15 mm, no other anomalies were detected and the correct treatment was prescribed, the prognosis is favorable - the baby may not experience any abnormalities.
An unfavorable prognosis develops if the size of the ventricles is more than 15 mm and dropsy grows intensively, the pathology is detected in the first half of pregnancy, multiple organ lesions are noted, which are characteristic of chromosomal diseases. The consequences of fetal hydrocephalus during pregnancy in such situations are quite deplorable - the death of a baby or serious damage to the central nervous system in a newborn.
Thus, a number of causes in the fetus and effective methods for detecting this pathology have been identified. Careful preparation for pregnancy and compliance with the recommendations for preventive ultrasound studies will help prevent the baby from getting sick.
In order to work normally and maintain the vital activity of the body, the brain must be protected from external negative factors that can damage it. The role of protection is played not only by the bones of the skull, but also by the membranes of the brain, which are the so-called protective case with numerous layers and structure. The layers of the meninges form, which contribute to the normal activity of the vascular plexuses, as well as the circulation of the cerebrospinal fluid. What are tanks, what role do they play, we will consider below.
Shells of the brain
The membranes have several layers: a hard one, which is located near the bones of the skull, arachnoid or arachnoid, as well as a choroid, called a soft sheet, which covers the brain tissue and fuses with it. Let's consider each of them in more detail:
- The hard shell has a close relationship with the bones of the skull. On its inner surface there are processes that enter the brain fissures to separate the departments. The largest process is located between the two hemispheres and forms a sickle, the back of which is connected to the cerebellum, limiting it from the occipital parts. At the top of the hard shell there is another process that forms the diaphragm. All this helps to provide good protection against the pressure of the brain mass on the pituitary gland. In some parts of the brain there are so-called sinuses, through which venous blood drains.
- The arachnoid membrane is placed inside the hard shell, which is quite thin, transparent, but strong and durable. It breaks the substance of the brain. Under this shell there is a subarachnoid space that separates it from the soft sheet. It contains cerebrospinal fluid. Above the deep furrows, the subarachnoid space is wide enough, as a result of which they form.
The meninges are connective tissue structures that cover the spinal cord. Without tanks, the brain and nervous system will not function.

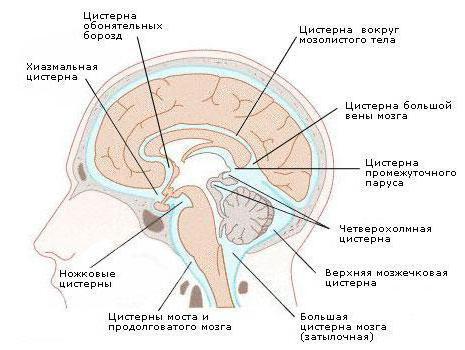
Types of tanks and their location
The main volume of liquor (cerebrospinal fluid) is placed in tanks, which are located in the region of the brain stem. Under the cerebellum in the posterior cranial fossa is called the large occipital or cerebellar-cerebral. Next comes the prepontine or cistern of the bridge. It is located in front of the bridge, bordering on the interpeduncular cistern, behind it borders on the cerebellar-cerebral cistern and subarachnoid space of the spinal cord. Further located. They are pentagonal in shape and contain such tanks as interpeduncular and crossroads. The first is located between the legs of the brain, and the second - between the frontal lobes and the intersection of the optic nerves. The bypass or bypass cistern has the form of a distorted canal, which is located on both sides of the legs of the brain, borders in front on such tanks as interpeduncular and bridge, and behind - on the four-colonial. Next, consider whether the four-hill or where is the retrocerebellar cisterna of the brain. It is located between the cerebellum and the corpus callosum. In her area, the presence of arachnoid (retrocerebellar) cysts is often noted. If the cyst increases in size, then a person may experience increased pressure inside the skull, impaired hearing and vision, balance and orientation in space. The cistern of the lateral fossa is located in the large brain, in its lateral furrow.
Cisterns of the brain are located predominantly in the anterior part of the brain. They communicate through the holes of Luschka and Magendie and are filled with cerebrospinal fluid (CSF).

CSF movement
The circulation of liquor occurs continuously. That is how it should be. It fills not only the subarachidal space, but also the central cerebral cavities, which are located deep in the tissue and are called cerebral ventricles (there are four in total). The fourth ventricle is connected to the CSF canal of the spine. The liquor itself performs several roles:
Surrounds the outer layer of the cortex;
Moves in the ventricles;
Penetrates into the brain tissue along the vessels;
So, they are part of the cerebrospinal fluid circulation line, they are its external storage, and the ventricles are an internal reservoir.
CSF formation
The synthesis of CSF begins in the junctions of the vessels of the cerebral ventricles. They are outgrowths with a velvety surface that are located on the walls of the ventricles. Tanks and their cavities are interconnected. B great cistern of the brain interacts with the fourth ventricle with the help of special slots. The synthesized cerebrospinal fluid enters the subarachnoid space through these openings.

Peculiarities
The circulation of cerebrospinal fluid has different directions of movement, it occurs slowly, depends on the pulsation of the brain, respiratory rate, and the development of the spine as a whole. The main part of the CSF is absorbed by the venous system, the rest - by the lymphatic system. Liquor is closely connected with the meninges and tissue, ensures the normalization of the exchange processes between them. CSF provides an additional outer layer that protects the brain from injuries and disorders, and also compensates for the distortion of its size by moving, depending on the dynamics, maintains the energy of neurons and the balance of osmosis in tissues. Slags and toxins are ejected through the cerebrospinal fluid into the venous system, which appear in the cerebral tissue during metabolism. Liquor serves as a barrier at the boundary with the bloodstream, it retains some substances that come from the blood and lets others through. In a healthy person, this barrier helps prevent various toxins from entering the brain tissue from the blood.
Features in children
The subarachnoid membrane in children is very thin. In a newborn child, the volume of the subarachnoid space is very large. As it grows, the space increases. It reaches such a volume as in an adult, already by adolescence.
Deformation of tanks
Tanks play a special role in the movement of liquor. Enlargement of the cistern of the brain signals a disorder in the activity of the cerebrospinal fluid system. An increase in the size of the large cistern, which is located in the small posterior cranial fossa, leads to deformation of the brain structure rather quickly. Usually people do not experience discomfort with a slight increase in cisterns. He may be disturbed by small headaches, mild nausea, blurred vision. If the disease continues to develop, it can lead to serious health hazards. Therefore, the synthesis and absorption of CSF must maintain a balance.
If a large amount of cerebrospinal fluid is collected in it, they talk about a disease such as hydrocephalus. Let's consider this question in more detail.
Hydrocephalus
This disease is formed when the cerebrospinal fluid circulation is disturbed. The reason for this may be an increased synthesis of cerebrospinal fluid, difficulties in its movement between the ventricles and the subarachnoid space, a failure in the absorption of cerebrospinal fluid through the walls of the veins. Hydrocephalus is internal (fluid is formed in the ventricles), and external (fluid accumulates in the subarachnoid space). The disease occurs with inflammation or metabolic disorders, congenital malformations of the pathways that conduct cerebrospinal fluid, and also as a result of brain injuries. The presence of cysts also leads to the appearance of pathological symptoms. A person complains of headaches in the morning, nausea, vomiting. There may be congestion at the bottom of the eye or swelling of the optic nerve. In this case, a tomography of the brain is performed to make the correct diagnosis.

cistern of the fetal brain
From the eighteenth to the twentieth week of a woman's pregnancy, according to the results of ultrasound, we can talk about the state of the fetal cerebrospinal fluid system. The data make it possible to judge the presence or absence of brain pathology. A large tank is easily identified using the axial scan plane. It gradually increases in parallel with the growth of the fetus. So, at the beginning of the sixteenth week, the cistern is about 2.8 mm, and at the twenty-sixth week its size increases to 6.4 mm. If the tanks are larger, they talk about pathological processes.
Pathology
Causes of pathological changes in the brain can be congenital or acquired. The first ones include:
AVM Arnold-Chiari, which occurs with impaired outflow of cerebrospinal fluid;
AVM Dandy-Walker;
Narrowing of the aqueduct of the brain, as a result of which there is an obstacle to the movement of cerebrospinal fluid;
Chromosome disorders at the genetic level;
craniocerebral hernia;
Agenesis of the corpus callosum;
Cysts leading to hydrocephalus.
Acquired causes include:
intrauterine hypoxia;
Trauma to the brain or spinal cord;
Cysts or neoplasms that disrupt the flow of cerebrospinal fluid;
Infections affecting the central nervous system;
Thrombosis of the vessels into which the cerebrospinal fluid enters.

Diagnostics
In case of violations in the cerebrospinal fluid system, the following diagnostics are performed: MRI, CT, examination of the fundus, examination of brain cisterns using radionuclide cisternography, and neurosonography.
It is very important to know how the CSF system works, how its pathology arises and manifests itself. In order to undergo a full-fledged treatment in case of detection of pathologies, it is necessary to contact a specialist in time. In addition, the results of ultrasound at different stages of pregnancy make it possible to study the development of the fetal brain in order to make a correct prognosis and plan treatment in the future.








